


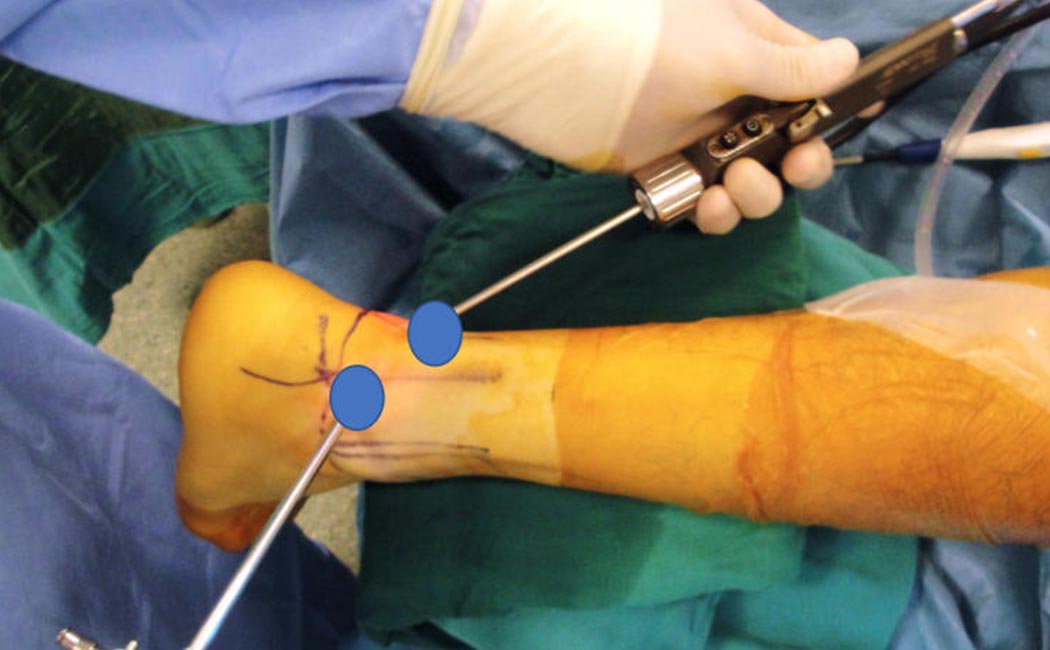
We can observe, examine and treat the bony and cartilaginous disorders in the posterior half of the ankle joint, a number of tendons, bony spurs on the heel bone (calcaneus) using the posterior ankle arthroscopy technique (Figure 1). Fiberoptics and surgical instruments are passed through 7-8mm buttonhole portals on each side of the Achilles tendon (Figure 2). The capsule covering the back of the ankle joint is very thin and is not a distinct structure like the capsule covering the front part of the ankle. The instruments used during surgery are passed through a fatty and fibrous tissue to reach the joint and a working space is created at the back of the ankle to visualize the structures and treat the pathology. Some problems like “Haglund’s disease” or Achilles tendon disorders do not involve the joint, but are located in this fatty area. Therefore the terms “arthroscopy” and “endoscopy” are used interchangeably for procedures in this location.


Posterior ankle impingement syndrome: A bony protrusion behind the talus bone (posterolateral process/Stieda process) or an accessory bone called “os trigonum” may cause a painful condition called “Posterior Ankle Impingement Syndrome (PAIS) (Figure 3). This disease is frequently observed in ballet dancers, dancers, soccer players who repeatedly force their feet downwards but can also be seen after an ankle sprain. The piece of bone or the protruding spur can be removed by posterior ankle arthroscopy for the definitive treatment.

Cartilage damage of the ankle: Cartilage damage in the back 1/3 part of the ankle may not be accessible using standard ankle arthroscopy techniques performed from the front of the joint. These are easily accessed with posterior ankle arthroscopy with the patient lying prone (Figure 4). Cartilage restoration techniques are routinely performed in this manner.

Subtalar joint cartilage lesions: The subtalar joint lies between the talus and the calcaneus and has limited mobility. This joint has a large cartilage surface on the so called “posterior facet” which can be accessed, visualized and treated arthroscopically. Typical small traumatic cartilage lesions can be trimmed to have an even surface and microfractured (small punctures on the bone to enhance cartilage regeneration) whereas degenerative lesions and end stage arthritis can be arthrodesed (fusion of the surfaces to make the two bones act like a single bone) (Figure 5). Ankle sprains, athletic trauma, falls from a height, rheumatological diseases are several of causes of damage in this joint.

Ankle arthrodesis (fusion): Fractures around the ankle, degenerative joint diseases, rheumatological disorders may lead to arthritis of the ankle joint. Fusion of this joint is one of the treatment options. Previous surgery, trauma, lesions of the skin and underlying soft tissues around the joint may sometimes leave the posterior (back) aspect of the joint a better option for surgery. Other technical considerations may also direct us to posterior ankle arthroscopy. Implants such as nails and/or screws are necessary to obtain fusion between the two bones, and the prone position during hindfoot arthroscopy facilitates the placement of these implants.
An overnight hospital stay is usually needed after hindfoot endoscopy. No cast or protected weight-bearing is necessary after soft tissue procedures and early range of motion exercises can be started. Return to sports is around 6-8 weeks. Fusion surgery takes longer to heal and a period of 6-8 weeks of protected weight-bearing with crutches is necessary. Your surgeon might also apply a short leg cast for a few weeks to immobilize the joint. Final healing may take up to several months.